



What better surgical data changes in a hospital
Structured surgical activity is not a reporting exercise — it changes how an OR runs, how surgeons train and how the institution spends.


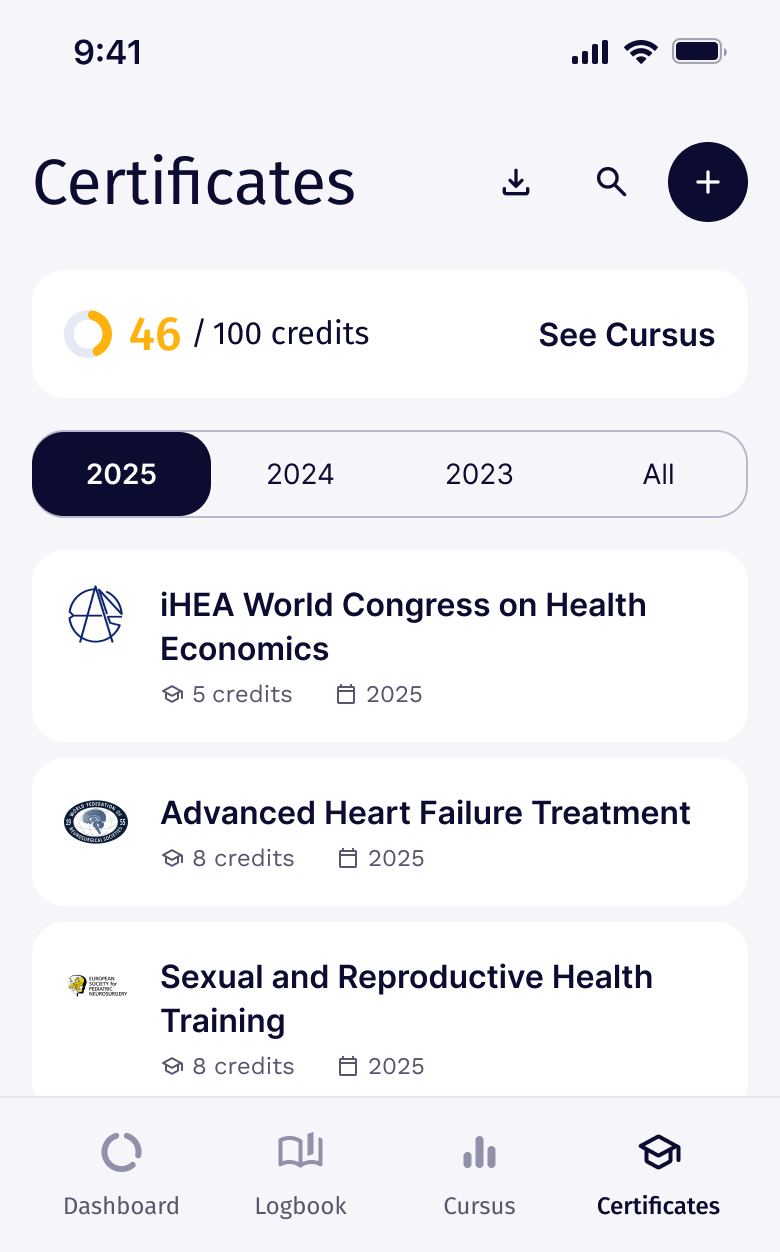
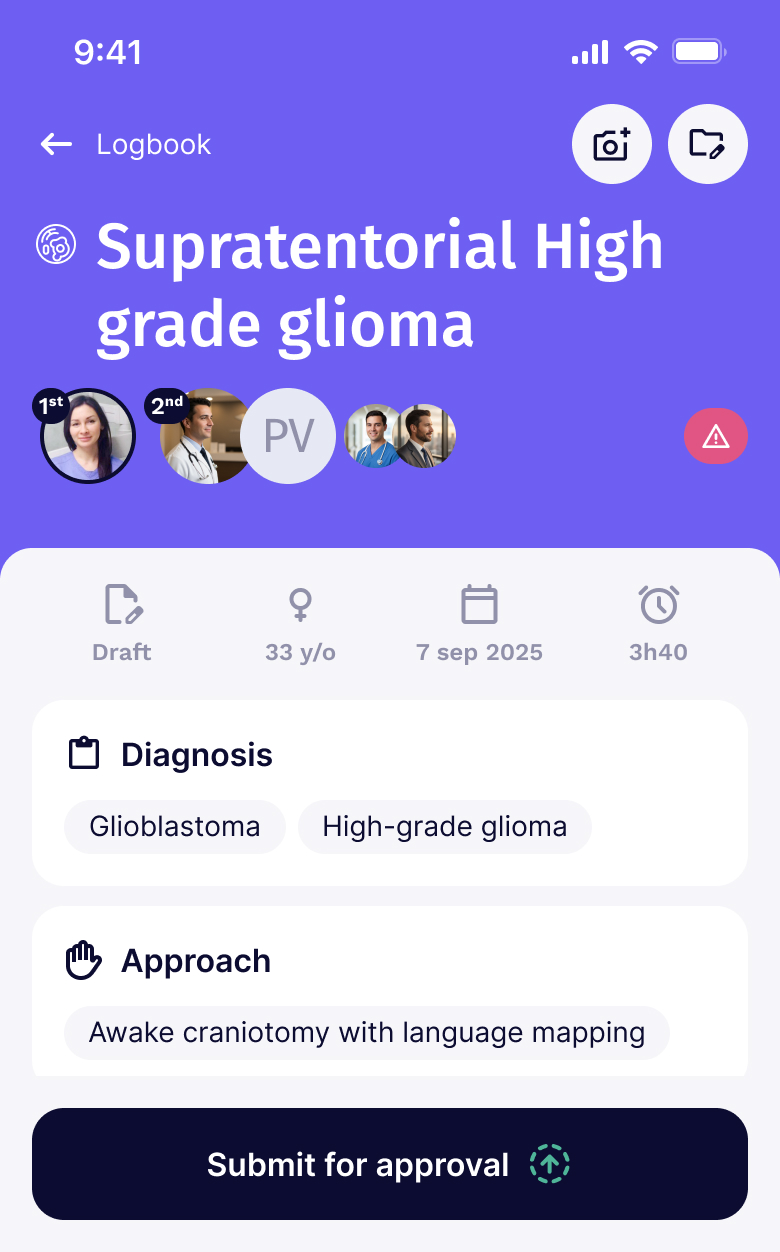
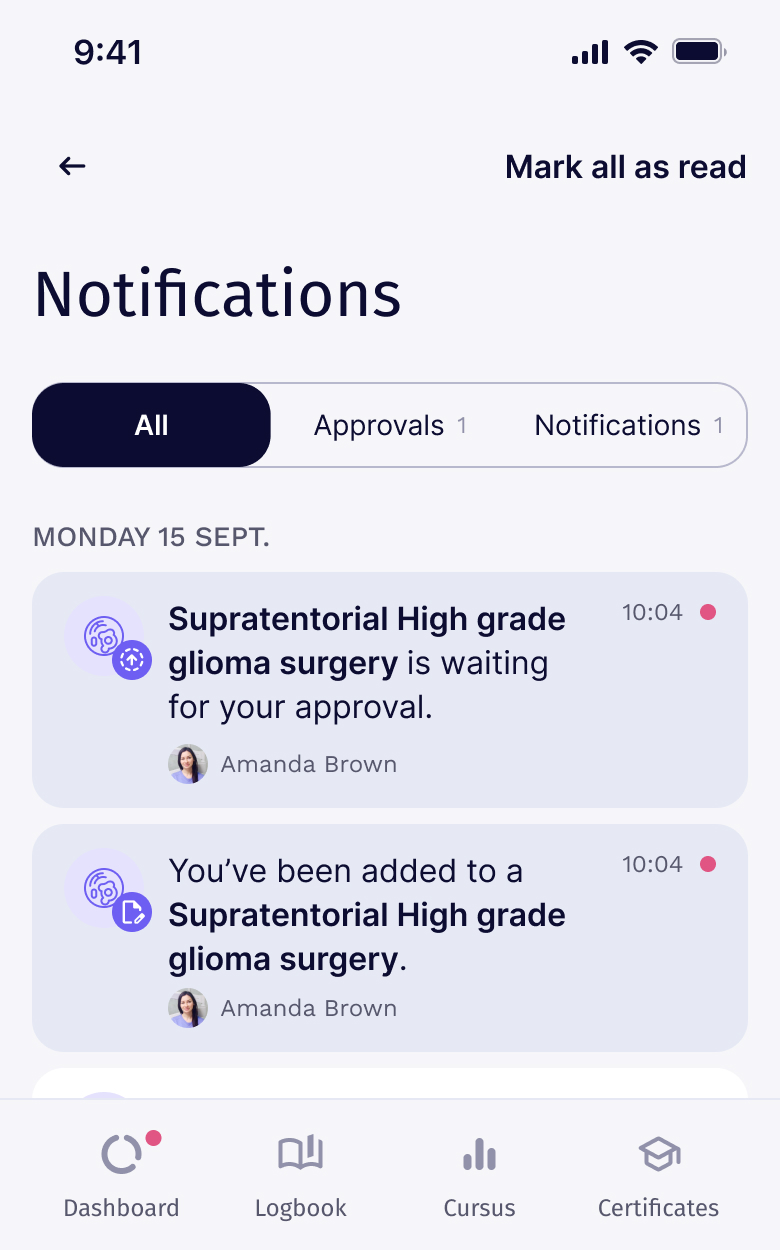
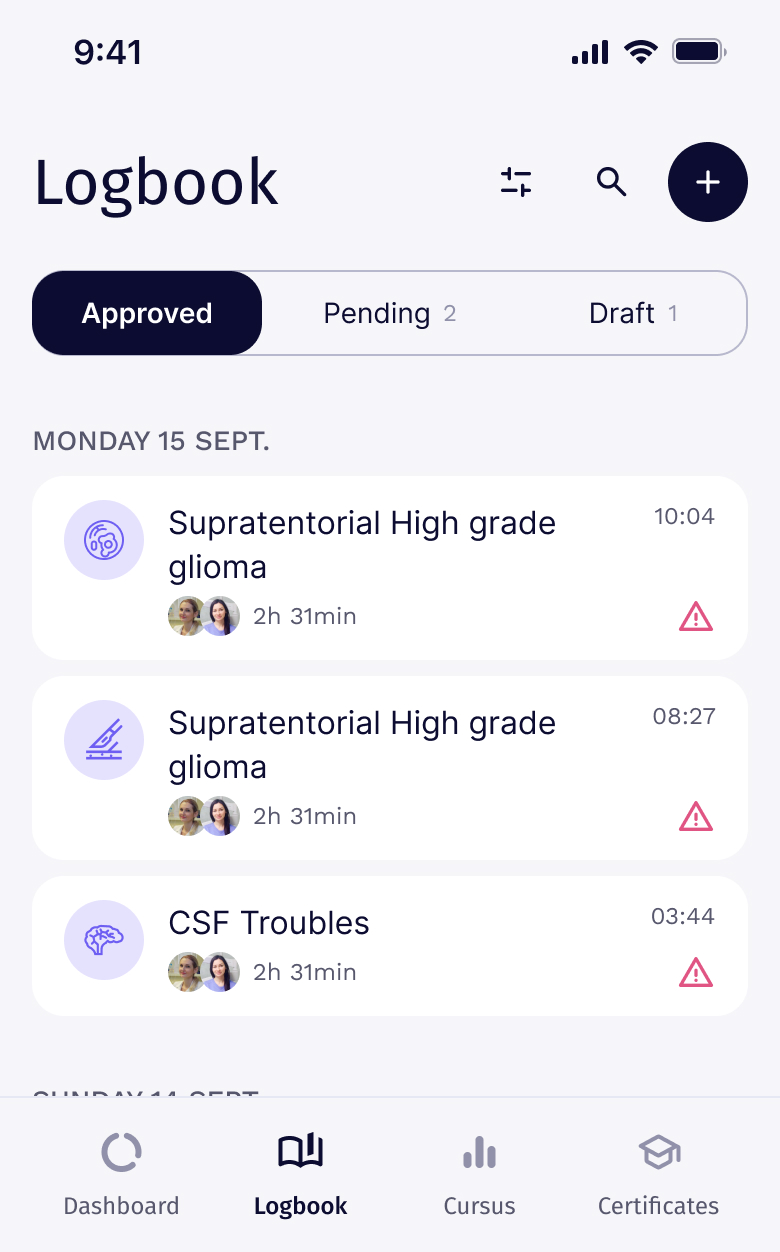
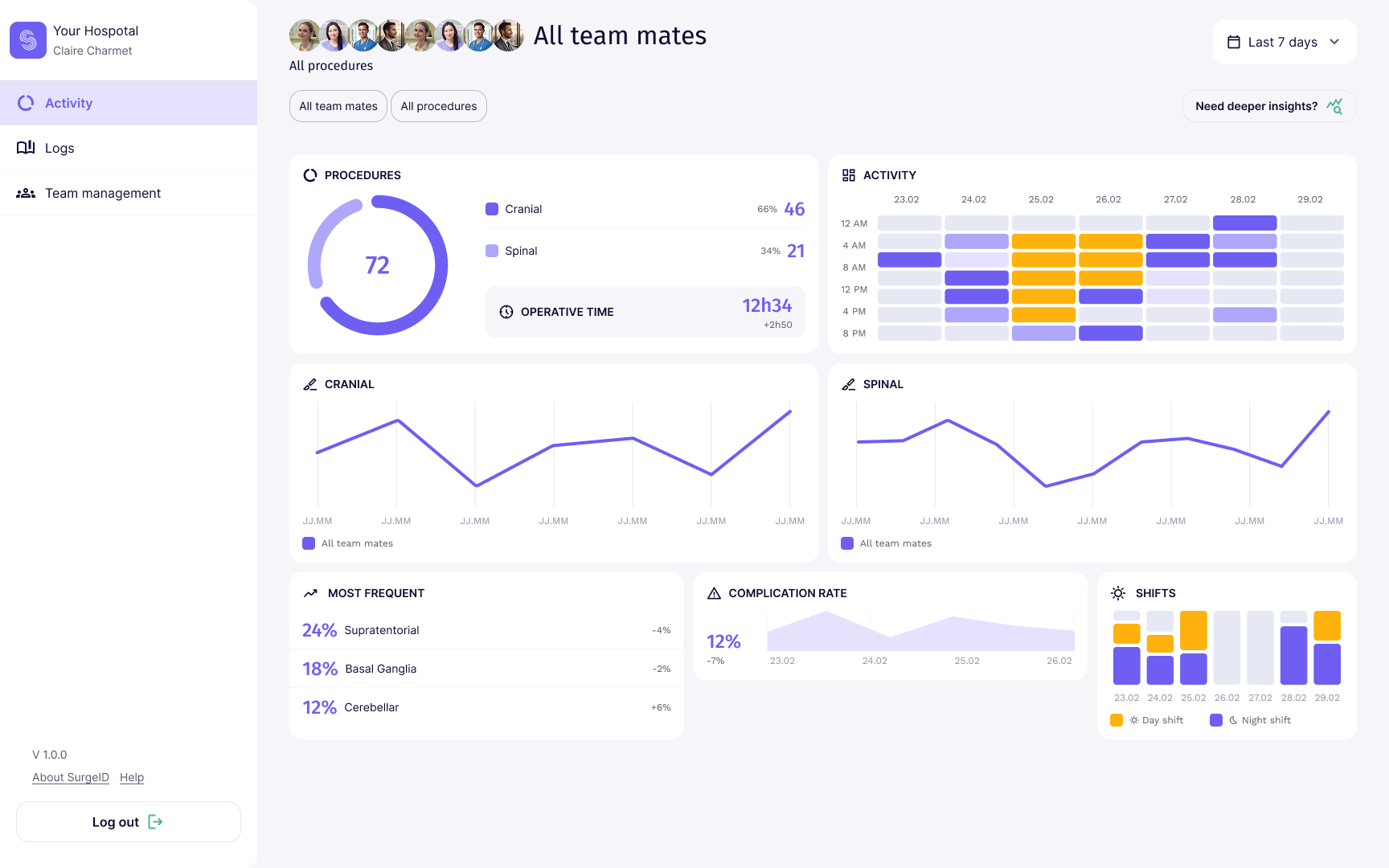
Real-time visibility on caseload, operative time, and team allocation. Surgeons spend less time on paperwork,hospitals plan blocks with actual data rather than estimates.
Complication and morbidity tracking at the procedure level. Patterns surface earlier, training gaps become visible,and outcomes improve through measurement, not assumption

Structured procedure data feeds directly into billing and insurance workflows, particularly relevant in fragmented systems like Switzerland (LAMal, LAA, complementary insurers). Less time on coding, fewer rejected claims, cleaner audits.
Our Vision
Surgical activity should be measurable, comparable, and reusable. Not as an administrative burden, as the raw material for better-trained surgeons, safer hospitals, and stronger clinical evidence. Surge-ID was created at the intersection of surgery, technology, and research to make that possible, starting in the OR, ending in the literature.
Our Team
Unique combination of Surgeons, engineers, and data scientists turning every procedure into structured, actionable surgical intelligence.

Neurosurgeon
Neurosurgeon


Attorney-at-law

Head of Investor Relations
Questions we get from surgeons, hospitals and industry
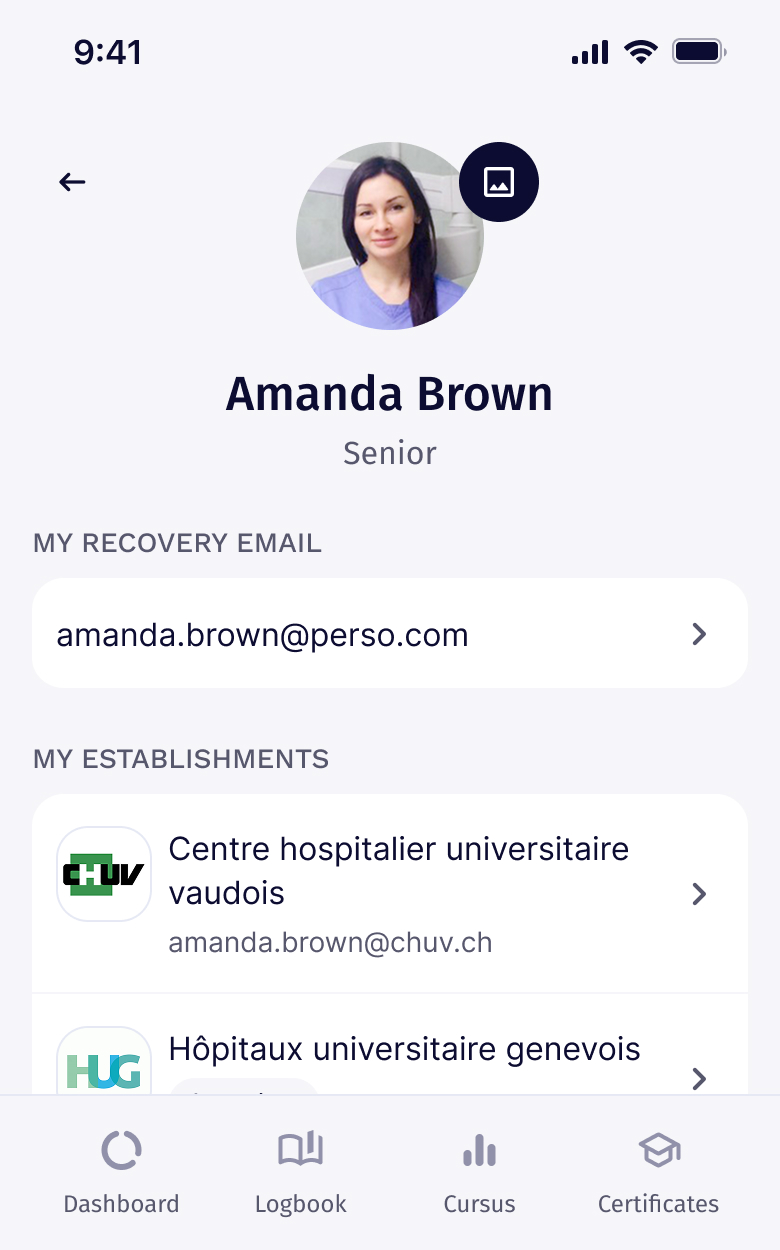
You do. Your logbook entries, certificates, and training records belong to you, not the institution. Hospitals see aggregate activity, not your personal portfolio.
Yes. Export the full record in standard formats when you change institutions. Continuity is a design principle, not a paid upgrade.
Standalone or alongside your HIS/EMR. Standard interfaces (HL7/FHIR) are available where needed; many departments start standalone and integrate later.
In Switzerland, the infrastructure complies with the Swiss Federal Act on Data Protection (nFADP) and GDPR. Hospital data stays within the institution's tenant.
A department typically goes live in 4–6 weeks: account setup, role mapping, light training, then production. No heavy IT lift.
The data structure, audit trail, and traceability are aligned with MDR PMCF requirements and FDA real-world evidence guidance. Documentation is available under NDA.
Yes. Run protocols across departments and institutions on the platform surgeons already use — no parallel CRF, harmonised data by design.
Patient identifiers stay inside the institution. Studies operate on de-identified, structured data; consent workflows align with local ethics committee requirements.